Political Economy of India’s Health Sector: The RG Kar Hospital Tragedy

Image Courtesy: PTI
‘Justice for RG Kar’, Kolkata, the ‘cultural capital of India’, has written new slogans reaching socially conscious academic spaces, especially the medical institutions of India. The slogans arose after a 31-year-old woman doctor was raped and murdered at her workplace, R.G. Kar Medical College and Hospital, in the heart of the city on August 9. At Esplanade, the historic centre of the city, a 17-day-long hunger strike was held that ended on October 21, with a promise from the government to set up a State Task Force to implement the demand of the protesting medical students.
The Junior Doctors’ Front – a leading body of the ongoing protest – has reasons to bring to the fore a much deeper crisis at their workplaces, beyond the issue of gender injustice in the tragic case. Therefore, the protest sites were brought out from the confinement of the gated premises of the medical institutions to public sites, where all walks of people joined in solidarity.
Famous film director, late Satyajit Ray, made a film on a tyrannical king of ‘The Kingdom of Diamonds’ (Hirak Rajar Deshe) as childhood entertainment for everyone. The film seems to have turned ‘real’ for the young protesting doctors. A solution, not just a short-term superficial paribartan (change) in the present crisis in the health sector, but a long-term structural transformation is required in West Bengal.
In Bengal, at present, there is a sense of disillusionment with the political claim of the promise of paribartan (made by the ruling regime) and increasing disgust at its franchisee politics, which was evident in the two months of the unbending protest. This feeling will not evaporate in the promise of forming a State Task Force, whose form, content, and timeline, i.e. terms of reference, are is yet to be officially published.
A logical and transformative solution for any problem lies in the questions being raised, such as: What led Abhaya (the victim of RG Kar, as named by the protesters) to be assigned 36 hours of duty? Is it not physically impossible to work for so long, and doesn’t this compromise the quality of health service being provided, which demands a high degree of cognitive attention, especially with regard to in-patient or intensive care unit (ICU)? Why did the hospital not have infrastructure and amenities, including security, as per the standard requirement of medical-institutions? Why is the right to dignified work and workplace for health workers and dignified care for patients both being compromised? The list of everyday indignities faced both by the citizenry and healthcare personnel is long.
The answers to these questions are intrinsically linked in the political economy of the health sector, whose consequences are revealed in the sub-standard health infrastructure, unprofessional security, overworked health staff, and deprivation of patients from quality care. The RG Kar tragedy, therefore, cannot be understood in isolation from the overall crisis in the health sector across India, and West Bengal, in particular.
Is India Undergoing a Healthcare Crisis?
The chapter titled “India’s Health Care Crisis” in the book, An Uncertain Glory, by economists Jean Dreze and Amartya Sen (2013) acknowledged that the Indian health sector had reached a crisis point decades earlier – perhaps over a generation. To comprehend the crisis, some key observations are worth highlighting.
Abhaya had been forced to overwork with a 36-hour-long duty. What could be the reason? Economists term this as a supply-side constraint in the number of health care staff, say, physicians in this case. Data shows that the Indian health sector is under-staffed, with 0.7 physicians per 1,000 population vis-à-vis 2.4 and 4.5 in China (a comparable country with India) and Germany (an advanced economy), respectively.
Had the physician-population ratio of India been at China’s level, the country would have had 3.4 times more physicians; and 6.4 times with respect to Germany. Hypothetically, therefore, had RG Kar Hospital employed at China’s level of 3.4 times more physicians than the present level, Abhaya’s duty would have been shared with more colleagues. If it were 6.4 times more physicians, as per the German standard, Abhaya would have worked for perhaps standard working-hours needed for healthcare safety from the cognitive-demanding jobs of doctors. Incidentally, the Supreme Court has constituted a 10-member National Task Force to streamline and regulate the working hours of medical professionals.
The next question that follows is: Why does the Indian health sector employ a lower number of physicians, vis-à-vis China and Germany? The reasons can be found in the level of government expenditure on health in these three countries. The data shows that average (per-person) expenditure on health by the Indian governments is $25, whereas China spends $362, and Germany $5,237 per person. Had the Indian health sector been funded adequately, say, 14.5 times more as compared to China, the abysmal situation of lack of industry-standard health care infrastructure, including workplace safety and security, could be improved, the acute shortage of healthcare staff could be reduced, and perhaps, Abhaya would have got a dignified working environment and would have been alive.
The daily indignities faced by overworked medical personnel, and lack of quality health care received by patients, are, therefore, a result of the decade-long neglect (or lack of priority) for the ‘right to health’ and universal access to quality healthcare by political establishment, business lobbies, civil society, media, and, most importantly perhaps, overlooked by the healthcare professionals themselves.
Lack of adequate public health expenditure is a consequence of a neoliberal economic policy that demands government expenditure to be low, thereby limiting funds in public health infrastructure and relegating healthcare services to private players to reap profits. The Covid-19 pandemic has taught us the importance of public health infrastructure and the inherent deficiency in the private sector in delivery of vaccines and healthcare at a global scale at a time when humanity needed these the most.
Status of Health Sector in West Bengal
To understand the status and standard of healthcare infrastructure (physical as well as human), quality of healthcare services, and their distribution across districts (to best of this author’s knowledge), demands a comprehensive post-Covid study, tracking the trends over a decade in West Bengal.
This notwithstanding the fact that the state’s health infrastructure abysmally lags behind the national average in basic indicators. The ubiquitous sites of overcrowded hospitals and overworked healthcare staff cannot escape our sight. The fact is that while a Primary Health Centre (PHC) is allocated for 32,505 population nationally, in West Bengal, an average 68,034 people depend on a single PHC.
Widespread infrastructural deficits in healthcare have been accumulated over decades due to low priority to public health in our public discourse, poor media attention and health activism, as well as lack in governmental accountability and policy formulation.
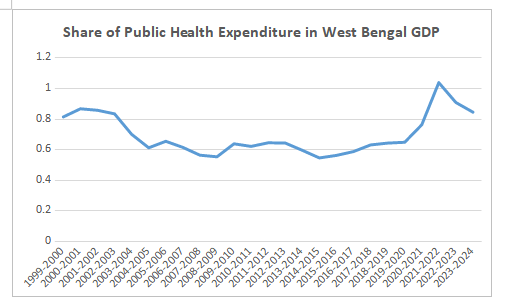
Amartya Sen has repetitively mentioned the health crisis in his findings, and cautioned us about the possibility of an ‘irreversible’ state of deteriorating public health, as vindicated by public finance remaining stagnant at very low level, below 1% of West Bengal GDP (gross domestic product) over decades.
The consequence of such acute deficits in healthcare provisions is reflected in overcrowded public hospitals with long queues of patients and their family. Some who have financial means travel to other states for OPD (out-patient) care or surgery. The remaining live with preventable morbidities, with hopelessness and distrust in the healthcare system. To best of this author’s knowledge, there are no statistics on the length of the queues, hours and days of waiting periods, number of people seeking healthcare outside of the state, and, most importantly, people being forced to live with preventable morbidities in indignity and hopelessness.
The State Task Force: What to be done?
The ‘Justice for RG Kar’ slogans were forceful enough to make the government agree to form a task force to address the 10-points demands of the agitating medical fraternity. As this agitation has grown without the leadership of any political party, and most importantly perhaps, without public-health specialised civil society members, the 10-point charter could not reflect the fundamentals of the crisis – the political economy of the state healthcare crisis – beyond merely emphasising some logistical issues, such as security and administrative concerns. Demand should not just be centred around lack of CCTV or centralised referral system.
This is not to say that industry-standard infrastructure and security provisions in medical premises are unimportant.
The medical fraternity has rightfully raised their workplace concerns and their compromised working conditions that deprive people of quality healthcare. Their two months of arduous agitation, with solidarity extended from people from all walks of life, has brought the government to the point of agreeing to form a task force, which was long due for 10.4 crore people of the state. Hence, in this regard, the vitality of this task force should set the standards after wide consultations. The form, content, and the timeline of the proposed task-force is important to give a logical conclusion to this movement.
The following points could be considered by the Junior Doctors’ Front and the broader medical fraternity to bring a transformative change in West Benga’s health sector:
The invited members of the task force should represent distinguished individuals from medical science, public health, health economists, legal counsels, workplace security experts, etc., not to mention representatives from the Junior Doctors’ Front.
-
The demand of task force should begin with preparing a rigorous and credible Expert Report on the Status of Healthcare in West Bengal within a reasonable timeframe.
-
All necessary administrative data and essential surveys on health and related subjects should be fast-tracked and financed, as necessary, by the government for building the Expert Report.
-
All necessary updates of the taskforce’s activities should be published on a public portal, say a dedicated website, to give the necessary information to the public and for transparency.
-
The task force should recommend the list of measures and public finance required for implementation of interventions.
-
Last, but not least, an independent social audit body needs to be constituted to monitor and audit the government’s interventions, and assess the improvement in the healthcare in a time-bound periodic interval.
These measures are easier said than done. Nonetheless, these are inescapable steps for bringing ‘Justice for RG Kar’ to its logical conclusion.
The writer studied economics from Jawaharlal Nehru University, New Delhi and taught at Tata Institute of Social Sciences. The views are personal.
Get the latest reports & analysis with people's perspective on Protests, movements & deep analytical videos, discussions of the current affairs in your Telegram app. Subscribe to NewsClick's Telegram channel & get Real-Time updates on stories, as they get published on our website.