






Global Health Crisis
Newsclick speaks to Professor David Sanders, founding Director of the School of Public Health, University of the Western Cape, about global health crisis. Professor Sanders says that even as many people talk about improvements in health levels globally, there is a growing inequality in health between the global north and south. This inequality is what Sanders refers to as the global health crisis. He further says that the world now sees the emergence of "diseases of development" along with the "old diseases" of poverty. While on one hand, children are under-nourished and stunted because of food insecurity and poor living conditions; on the other, chronic diseases related to "modern diets" are seen to be affecting a large population. In order to mitigate the effects of the crisis, Sanders suggests government intervention in the food trade by way of imposing taxes on unhealthy foods and subsidizing healthy foods. He says that global health movements can play a huge role in improving health standards, but attracting the youth into such movements will be a challenge.
Transcript:
Amit Sengupta (A.S.G): Hello and welcome to the Newsclick. Today, we are in conversation with Prof. David Sanders, Professor Emeritus at the University of Western Cape in the School of Public Health. Thank you David for being with us. Now, we would like you, given your vast experience in this area, to tell us about what in many quarters is being talked about as the Global Health Crisis. Now, why do we say it is a crisis and what are it's dimensions?
David Sanders (D.S): Thanks for having me. What many people do not talk about the global health crisis, many of the UN agencies point out with some truth that in fact health globally is better than it has ever been. That mortality rates have dropped faster than ever before.
A.S.G: And all true?
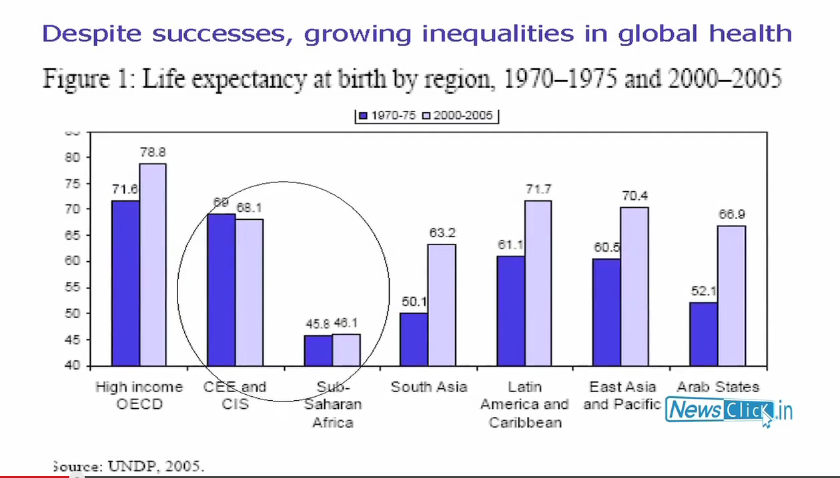
D.S: That is true except for some regions. So in some regions of the world notably sub-Saharan Africa and the former Soviet Union there has been a slight increase in mortality in Soviet Union especially in men and in Africa, there has been a virtual stagnation, no increase in life expectancy.
A.S.G: So this Soviet Union is post the demise of the socialism?
D.S: Yes. So what they don't talk efficiently about is the fact that there are also unprecedented inequalities in health and that’s really what the crisis is because it is very clear that some segments of the society in many countries, most countries actually, are achieving very good health outcomes. High life expectancy, living longer than ever before, lowering, extremely low young child mortality in some of the richer countries and some of the middle-income countries but huge inequalities between North and South which have increased dramatically. For example, young child deaths under five, mortality, there was a ratio about thirty years ago of 9:1 between global South and North in terms of rates. So it was nine times higher in the global south. 30 years on, 27 fold difference. So there has been extreme widening of the gap between North and South and within the countries, a widening of the gap. So for example, in a country like India, under five mortality in the richest quintile of the population is about a quarter of that in the poorest quintile.
A.S.G: So you are saying that the gap is increasing but overall there is an improvement in health. So if someone were to argue that in the long term this would mean that finally everybody would be healthy. What would be your response to that?
D.S: That's highly unlikely because of what we are seeing especially in the global south and to some extent in the global North as well. We are seeing the emergence of diseases of “development” by which I mean heart diseases, metabolic disorders like diabetes, cancer along side the old diseases of “poverty”. I put these in inverted commas because actually the poor are now also experiencing early onset of diabetes, heart diseases and so on while at the same time, their children suffer from infectious disease, morbidity, and old infectious diseases. So we are seeing in a sense a dual pattern on many levels. We see dual pattern between countries where in the advanced countries there has been a transition to these non-communicable disease or be it with disparities between rich and poor and growing ones. But in Southern countries, many countries are not making that transition or to be more precise, many sectors of those populations are not making that transition.
A.S.G: You said earlier that this is a global phenomenon more or less. In which case are there any structural factors at the global level, which can explain this growing disparity and vulnerable communities that seem now to be trapped in a cycle and they are finding it very difficult to escape out of it?
D.S: Yes, there are of course structural factors. One can conceive the factors the result in these disease patterns as, to use a metaphor, almost like a stream. So we can think of the downstream causes, which are the immediate biological causes all the way up to most distal or upstream causes such as the global economic structures. So to give an example, we find that many of the old type of infectious diseases are underpinned by under nutrition. So under nutrition remains rife. In fact one in four children globally is stunted, chronically undernourished. Yet world food production is at an unprecedented level. Even in India, there is a surplus of food and yet there continues to be very high percentage of children who are extremely undernourished. So then we have to ask, ’why is it that amidst plenty we find this persisting problem of chronic food insecurity and infection?’ Well, it is because the living conditions and purchasing power of poor people has not really improved and there are factors that control the global food supply which make it more and more difficult for poor people to get adequate diet. On the other side to use the nutrition analogy we are seeing more and more chronic diseases related to 'modern diets'. So diets which consist increasingly of processed foods, fast foods, foods which are high in calories with refined carbohydrate and fat, very salty and these tend to produce problems like diabetes, high blood pressure, heart disease and so on. We find the poor are now also increasingly purchasing such diets because they are cheaper. They require less cooking, less time and they are convenient and tasty. So using nutrition, we can see that there are downstream factors, what people eat and upstream factors, the structural dimensions which determine these and these are increasing as fast food is concerned, driven by liberalised agriculture and food trade and a sector increasingly dominated by few and fewer very large transnational food corporations.
A.S.G: Are you saying that this is somehow related to the structure of capitalism today?
D.S: Absolutely.
A.S.G: How do you actually counter these trends? Now if these are structural factors, one response would be that we need to reverse the neo-liberal ideological penetration into policy making across the world. But concretely in the health sector, are there other methods one can use at least to mitigate the impact of these policies?
D.S: It would be possible for governments to intervene in the food chain to promote better diets. So for example, governments could, although it won't be without resistance we have seen in many countries, impose taxes on unhealthy foods, for e.g. sugary beverages, and at the same time subsidise healthy foods. Of course, it is extremely complicated as we saw recently in New York. There was an attempt to limit the volumes of sugary beverages sold so as to try and reduce the size of what people could purchase. This went through the legislation but the soft drink companies took the mayor of New York in this case to court and they reversed that. This is in the most powerful country in the world in a way. So it is extremely difficult for the countries to do this but they can do this. In Brazil for example, there is a big policy intervention Bolsa Familia, which is conditional cash transfer. So that conditional cash transfer is given to poor people and much of it goes into purchasing food. So there are other interventions, which try to ensure a better food environment. For example, the school feeding programme in Brazil. A recent legislation passed in Brazil states that 30% of all school food needs to be sourced from local small producers and needs to be fresh food. So there are ways governments can intervene although governments are of course extremely restricted by WTO undertakings.
A.S.G: In the health system, are there are any interventions that are possible even within the constraints that we have. I am also asking in the context of the range of public services, which are today being dismantled. This is not just happening in the global South but also in the global North where earlier it was taken entirely granted. So we have a trend of public services being dismantled, health services being one of the key ones which are under attack. Is there a response possible to turn back this tide?
D.S: Well, the first battle that needs to be won is to confront the assertion. It's mostly an ideological position that the private sector is most efficient and effective. So for that we need evidence. There is some evidence showing that where the countries where public sector health dominates health outcomes are better and there were countries where private insurance,
A.S.G: Like?
DS: Well, for e.g. Costa Rica, of course, Cuba is unusual as you know because of its political system but there are also countries whose economies remains capital but the state intervenes in the social sectors. Costa Rica is one, Thailand is another and there are some other smaller African countries. Brazil is an example although in Brazil there are huge disparities in private sector where the state controls the sector. They have very some thoughtful policies such as some of that I have mentioned where they intervene to ensure, better and more accessible health services. So in relation to nutritional problems Brazil has managed to reduce child under nutrition.
A.S.G: But international agencies today, many of them, are arguing that it does not matter which cat catches the mouse as long as the mouse is caught. In other words, it does not matter whether provision of services is by the private sector or the public sector and all their governments need to do is to regulate the health sector and see that everybody behaves properly. Is that something that you would agree with?
D.S: Well, there is a lot of evidence privately funded or worse, private services funded from the public purse or a great team or expensive and less cost-efficient than well functioning public services. So of course, one of the problems including India is that public services don't function very well by and large. So in the countries where public services have been invested in and specially the human resource component in public services at all levels, from the policy level to the service delivery level, have been invested in by which I mean, enough people in the right places of right skill then we see very good health outcomes, especially in countries where the public sector dominates.
A.S.G: So we have talked about structural issues that need to be actually addressed including the structure of capitalism itself and about the need for reform in the health sector of a different kind, of bringing back the public. Now, since you are one of the founders of the Peoples Health Movement, what roles do movements play in making a difference?
D.S: There is absolutely a fundamental role. If ones looks at the history of health improvement going back even to 19th and early 20th century where the UK is the best known case because statistics were kept there almost earlier than anywhere else. They were kept from about 1840. If you look at the improvement in health in UK, it really preceded any effective medical measures like antibiotics. It improved because living and working environments improved including better, more reliable, more equitable food supply, eventually better water sanitation and better working conditions. But these did not happen simply because legislation came into being. Preceding and accompanying the legislation were huge struggles by people. There were struggles in London during the cholera outbreaks during the 1830s. There were struggles against exploitative and dangerous working conditions. The formation of the trade union movement and later the labour party among other struggles led to reformers being thrown up and reforms being enacted to essentially introduce public health legislation as we call it. Of course, the UK's path can't so easily be followed because the UK at that time was a major imperial power and was deriving a lot of wealth through colonial exploitation. It was the factory of the world and great wealth was being generated and redistributed to some extent through popular struggles. But there have been later examples. Brazil slightly before the end of the dictatorship enacted on the basis of huge popular mobilisations, a whole number of new social policies. So the architects of Brazil's Health policy were people who were involved in the struggle against the dictatorship. There are many other examples, which did not last long. Like in Zimbabwe for example, where in the wake of the National Liberation Struggle and great pressure from the population, there were many social reformers enacted. The economy remained capitalist but the government invested heavily in health, education and other social areas and there were rapid improvements in health. Sadly because history does not move in a straight line, much of that has been turned back.
A.S.G: Last thoughts. Do you see emerging global movements, although fragmented, as positive outcomes of globalization and as something in the belly of the beast that could actually change the situation?
D.S: Yes, I do. I have been teaching in universities for over thirty years and have encountered a lot of young people coming into public health. Of course that is a biased sample because those who go in to public health are almost self-selected. But I do see over the past decade and probably accelerating, more and more interest in the some of the ideas we are talking about.
A.S.G: Why is it so?
D.S: I think it’s because young people see for themselves extremely bleak futures if the current status quo persists. They see their peers emerging, even with tertiary education, unable to get jobs. They see misery around them even if they are in so called advanced countries. They see conflict around the world, which is now even impacting them. And some of them have started asking questions. They are asking questions about whether what is proposed really offers a way forward. In that sense there is a big opportunity for progressive movements to grow. I don’t think that progressive movements have yet found exactly the correct formula because the objective situation is really critical. Yet we see with some exceptions not many movements on the ground. We see movements such as the Occupy Wall Street movement, which peak and defervesce. We see some mobilisations on the streets by Spanish youth, more than 50% of who are unemployed but we don’t see a sustained movement.
A.S.G: But you do see that we are starting to get there?
D.S: I see much bigger opportunities. I see a lot more interest in People’s Health Movement and associated movements. I think the big challenge is for these movements to be more attractive than they are presently, especially for the youth and for the movements to start to connect to each other because ultimately the root of all problems is the same; unequal, unsustainable economic and political system.
A.S.G: Thank you David.
D.S: Pleasure.
Get the latest reports & analysis with people's perspective on Protests, movements & deep analytical videos, discussions of the current affairs in your Telegram app. Subscribe to NewsClick's Telegram channel & get Real-Time updates on stories, as they get published on our website.















