






Covid-19: It is Not the Money but the Intention that Counts in Healthcare

The first cases of Covid-19 were seen nearly eight months ago in China. Since then about 1.5 crore people have tested positive for the disease worldwide, and of them more than six lakhs have died. The actual numbers may be higher, as many of the infected have not been tested. The disease has no cure. “Testing, tracing and isolation”, first recommended by the WHO on 18 March, are the only medical interventions being followed the world over. However, the spread and fatality rates of the disease are markedly different across countries, even those with similar economic and climatic conditions and population age profiles. The administrative failures of a Trump or Bolsonaro are one factor. Surprisingly, little attention is being paid to what is perhaps the most important reason, a country’s healthcare system.
A naïve popular belief is that richer countries have better healthcare systems and healthier citizens; hence their people are better protected in a pandemic. Supposedly sophisticated research also arrives at a similar conclusion. A Global Health Security Index developed at the John Hopkins University last year to specifically check the readiness of different countries to identify and contain an epidemic gave the United States, the country with the maximum per capita expenditure on health, the highest rank. Contrary to this assessment, the United States tops the list of infections and deaths due to Covid-19. A healthcare system is not just a storehouse of medical resources and a passive conduit to deliver them to citizens. Through its guiding philosophy and organising principles, it selects those it serves and the diseases it prevents and treats. Hence it should not surprise if a country’s healthcare system has no bearing on the spread of Covid-19.
The following table lists the data on Covid-19 spread, healthcare systems, life expectancy and per-capita incomes in a few selected countries, as indicative of the nature of their health systems, including the general health of the population and availability of economic resources.
Table: Covid-19 Spread and Healthcare Systems in Selected Countries
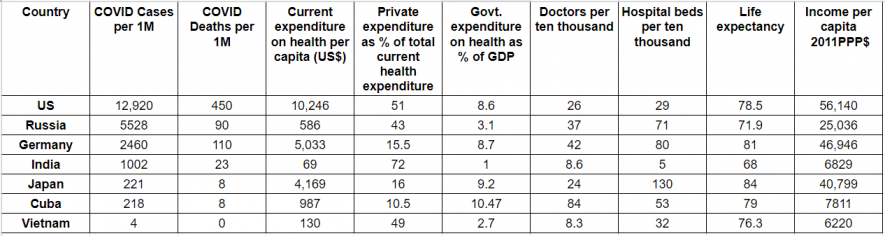
Data sources: Worldometers.com, WHO, HDR 2019.
As seen in Table 1, the United States, which has the highest income among the listed countries, has the highest infection rate and deaths per million due to Covid-19. Russia has less than half the infection rate of the United States. But its fatality rate is five times lower. Russia has conducted more tests per million than most large countries, and also has more doctors and hospital beds per 10,000 population than the United States.
Vietnam has the lowest income among the listed countries, but also has the lowest spread of Covid-19. In fact, no one has died due to the disease in Vietnam. The country shares a 1,300-km border with China where the disease originated, and was among the first to report the infection. The very low spread of the disease in Vietnam can be attributed to the preventive measures its government took. Also note that despite spending 70 times less per capita on health than the United States, it has a higher number of beds per 10,000 people, and hence is able to provide greater institutional support to the ill.
The healthcare systems of countries have evolved through their histories and therefore vary greatly in terms of priorities, coverage, sources of funding and operating protocols. Not all nuances of a healthcare system can be captured by quantitative data. Nevertheless, certain distinguishing features are clearly visible. Cuban healthcare enjoys maximum state support. Government expenditure on health as a percentage of GDP is the highest in Cuba, and its private expenditure on health is the lowest. Similar characteristics are seen in Germany and Japan. All these countries have a higher life expectancy and have done a better job of containing Covid-19 than the United States, even though their per capita expenditure on health is lower than the latter’s.
Cuba’s case is the most remarkable as it spends only one-tenth per capita on health than the United States, yet provides better health care to citizens.
India and the United States have the most privatised health systems. Nearly three-fourths of the health expenditure in India is private. In the United States, even though nearly 50% of the expenditure is made by the government, the actual delivery of health services is in private hands. A comparative analysis of Vietnam and India is also instructive. Both are middle-income countries. The per capita income of Vietnam is 10% percent less than India’s. Yet the country spends two times more per capita on health than India. As a percentage of GDP, the government of Vietnam spends nearly three times more than India on health. This difference shows up in the health outcomes: an average Vietnamese lives eight years longer than an Indian.
The data in the table clearly show that the health care systems of different countries are producing very different results in terms of health outcomes and containment of COVID 19. Per capita expenditure on health is not the key factor. Higher public expenditure on health, both in richer and not so rich countries, leads to better outcomes. Public expenditure though is itself a result of social values and what is expected from a good health system. Another factor is the organisational principle of the system, which determines how and in what form available resources are distributed. The following section provides a closer look at these by comparing the Cuban and US healthcare systems.
Social care versus monetised service in Cuba and the United States:
Healthcare systems in Cuba and the United States are driven by contrasting philosophies and organising principles. Cuba has a community-based public health system which is designed to be equally accessible to all, and is practically free. It is an integral part of the Cuban state’s governance structure; hence the social base, ideology and politics of the Communist Party of Cuba play a very important role. The United States has a privatised health system in which every service is charged for. Insurance companies, large pharmaceutical corporations, hospital management and highly-specialised medical professionals play a key role in this system.
Access to decent health care is accepted as a fundamental right in Cuba’s Constitution. It is planned with the intention that within the resources of the country, it should be accessible to all at their doorstep at no personal cost. Che Guevara, a doctor himself, played an important role in establishing it after the Cuban revolution. Fifty five years after his departure, the system still bears the stamp of his radical egalitarianism and humanism. Health care is seen as an essential provision of what is needed by the ill, rather than a transaction.
At the base of the Cuban health system are the family physicians and nurses in neighbourhood clinics. One physician and nurse typically take care of 120 to 150 families. They live in the neighbourhood, among the people they serve. Besides providing round-the-clock care to the sick, they keep tabs on everyone’s health through regular home visits and surveys. Upper levels of the system are composed of polyclinics, which serve between 20,000 to 60,000 people, and regional and provincial hospitals. The emphasis is on distribution of human and material resources to neighbourhoods and villages, rather than their concentration in bigger cities. A conscious decision has been made to create skilled human resources who can intervene on the ground, rather than importing expensive diagnostic machines. As the data in the table shows, Cuba has highest number of doctors per 10,000 people, three times more than the United States and twice as many as Germany.
The Cuban health system gives top priority to disease prevention; so the training of medical professionals, and protocols emphasise pro-active measures. Since every Cuban is linked to the health delivery system at its base, identification of people at risk, population-wide vaccinations and transmission of necessary instructions is relatively smooth. The system generates a high degree of mutual trust between people and health care providers, and a high degree of public awareness about health issues. It has regularly responded well at times of natural disasters like the annual hurricanes and threat of epidemics such as dengue and HIV-AIDS. It has also been remarkably successful in eradicating diseases of poverty such as polio, tuberculosis, malaria, diphtheria and measles by shifting into campaign mode.
The health system in the United States is more like a consumer-delivery system, under which health products and services are differentiated, monetised and made available at a price. Hence the system has a transactional character, which affects the behaviour and expectations of both service providers and receivers. The state provides financial support to programmes for health needs of the worst-off cases, for example, the senior citizens, poor children, pregnant women, and the disabled. Most people depend upon private health insurance, which they buy on their own, or it is linked with their employment. The country spends 16% of its GDP on health, which is the highest in the world. While the state expenditure on health is nearly 50% of the total expenditure on health care, the actual delivery is with private entities. Even state-supported health services are managed through private agencies. The commercial logic of the system is to lower its own costs while jacking up prices receivers pay. For example, the number of hospital beds—25 per ten thousand—is less than even much poorer Vietnam or Cuba. The system gets activated only after illness and there is little built-in motivation for prevention.
On the surface it would appear as if individuals in the United States decide how and where to access health services. In practice, their system leaves everyone to their own devices, and immense economic, racial and regional inequalities are reproduced in the access to health. According to United States Census reports, 8.5% Americans (around 25 million people) did not have any health insurance at any point during 2018. Paradoxically, these people, who are among the poorest Americans, are also the most likely to face the maximum health-related problems. Even for those who can access the system, there is little uniformity in quality and delivery. Multiple layers of insurance related red-tape, and state policies mean that the system has high internal costs and friction, and there is little scope for coordinated action. And this is the situation during normal conditions. The system fails miserably when there is a sudden shock. Hurricane Katrina in Louisiana in 2005 left hundreds of thousands of poor African-Americans without basic health services for weeks.
The shock of Covid-19 has been exacerbated by the loss of employment due to the lockdown and consequent loss of health insurance for many, which made them reluctant to seek medical aid. Since the health system largely leaves everyone to their own means, it generates little public trust and awareness of health issues. In the case of Covid-19, this has made contact-tracing and the isolation of infected people nearly impossible. People are reporting to hospitals only when their condition is critical, overloading the already stretched system.
Pathogen-induced diseases and their cures by vaccinations or antivirals and antibacterials are objective processes determined by the natural laws of biology and biochemistry. Any health system, however, is a value-laden structure created by society. After a cure is found for Covid-19, it is very likely that healthcare systems everywhere will fall back to its normal state. However, 15,00,000 humans die every year due to tuberculosis and 400,000 due to malaria, under such “normalcy”. Three hundred thousand women die every year during child birth. In India alone, around 100 women die every day during child birth. Most of these lives can be saved if the healthcare systems stops discriminating on the basis of wealth, race, gender or caste, and is organised around the principle of human needs rather than private profit.
The author teaches physics at St Stephen’s College, Delhi. The views are personal.
Get the latest reports & analysis with people's perspective on Protests, movements & deep analytical videos, discussions of the current affairs in your Telegram app. Subscribe to NewsClick's Telegram channel & get Real-Time updates on stories, as they get published on our website.















